The purpose of this course is to provide an overview of breast cancer, its risk factors, clinical features, common subtypes, and treatment modalities, including a detailed review of the most commonly used systemic treatments, including prescribing indications, side effects, and warnings based on updated clinical evidence, and a brief summary of early detection and screening guidelines to enhance APRN practice and improve clinical outcomes.
...purchase below to continue the course
t with a BRCA1 or BRCA2 mutation has a 50% chance of inheriting the same gene mutation (US National Library of Medicine [NLM], 2020).

Pathophysiology
As demonstrated in Figure 2, breasts are composed of epithelial, stromal, and adipose (fat) tissues. Glandular tissue includes the ducts and lobules. Each breast contains about 15 to 20 lobes, which has many smaller subsections called lobules. The lobules lead to bulbs that generate milk, and all of these components are linked together by thin tubes called ducts. The majority of breast cancers arise from the cells forming the lobules and ducts as carcinoma in situ, which is an early-stage, noninvasive, abnormal proliferation of cells confined only to the ducts and lobules. The lymphatic vessels of the breast flow in the opposite direction of blood flow, and they drain into lymph nodes. It is through the lymphatic vessels that breast cancer cells have the opportunity to metastasize (or spread) to lymph nodes. Most lymphatic vessels flow into the axillary lymph nodes, which are located under the arm. Understanding the patterns of lymphatic drainage is essential, as when breast cancer metastasizes, it usually involves the first lymph node in the chain of lymph nodes (McCance & Heuther, 2019).

The pathophysiology of breast cancer is complex and multidimensional. Breast cancer is a heterogeneous disease with various molecular, genetic, and pathologic alterations. Breast cancer subtypes are classified by their specific clinical features, including histology, anatomical origin, tumor staging, hormone receptivity, and human epidermal growth factor receptor 2 (HER2) expression. The three most common types of receptors known to fuel most breast cancer growth include the estrogen receptor (ER), progesterone receptor (PR), and the HER2/neu gene expression. Awareness of the presence or absence of these receptors is vital to determining the most optimal, evidence-based treatment regimen. Overexpression of HER2/neu is associated with poorer overall survival rates, especially in patients who have lymph node metastasis (Masoud & Pages, 2017). The most common expression status of breast cancer is hormone-receptor (HR)-positive, HER2/neu-negative. While there are several types of breast cancer diagnoses, the major subtypes are explained in Table 1 (Watkins, 2019).



Signs and Symptoms
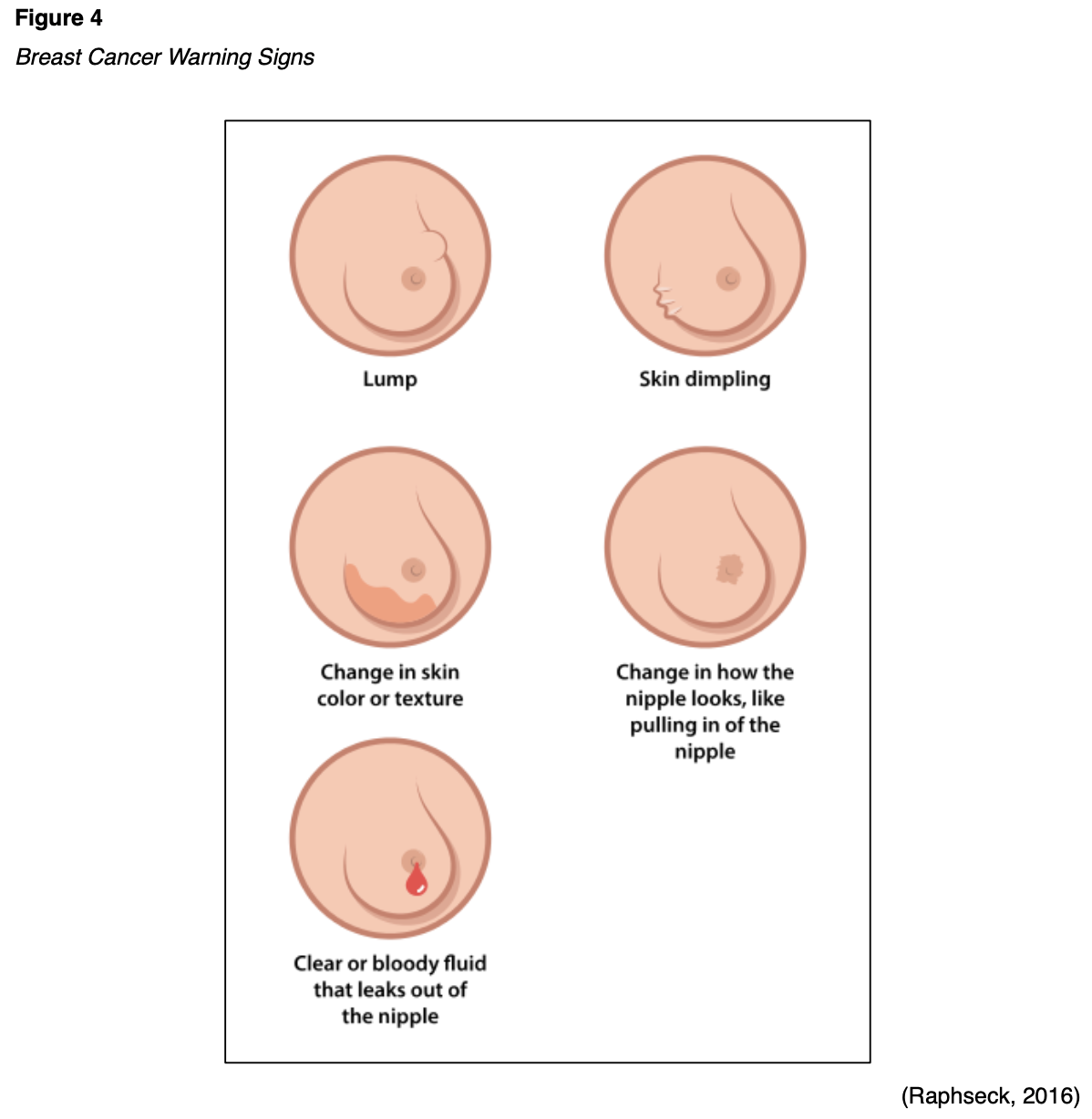
Early breast cancer generally has no signs or symptoms due to its small size and is most commonly identified on routine screening with mammography. If the breast tumor grows large enough, the most common signs include a unilateral, palpable mass with irregular borders. It may be a painless lump that is immobile or fixed to the skin and may or may not be accompanied by enlarged axillary lymph nodes. Some women may report changes to the breast caliber, texture, or shape, including asymmetry or open wounds or lesions that arise spontaneously. As demonstrated in Figure 4, skin changes such as retraction, thickening, or dimpling of the skin on the breast may also occur. Nipple changes may also occur, including retraction of the nipple or spontaneous discharge. Blood or purulent discharge expelled from the nipple is an ominous sign of underlying pathology (Nettina, 2019).
Diagnostic Imaging
Most breast cancers in the US are diagnosed through mammography screenings. Mammography and ultrasonography are the most common breast imaging tests. As demonstrated in Figure 5, mammography uses low-dose x-rays to view inside the breast as a means to identify abnormalities suspicious for breast cancer. A standard mammogram is equivalent to approximately seven weeks of natural background radiation. In modern medicine, mammography is performed as a screening modality (to be discussed later) or as a diagnostic test. Diagnostic mammography is performed as a follow up to an abnormal screening mammogram, or in patients who present with suspicious breast abnormalities, such as a palpable breast lump or skin changes. Diagnostic mammography differs from screening mammography in that it is supervised by a radiologist to tailor the additional views toward the area of suspicion to better characterize the abnormality, and a breast biopsy is commonly advised for highly suspicious findings (Koh & Kim, 2019). Diagnostic mammograms have lower sensitivity in women with increased density of the breast tissue and cannot differentiate between solid or cystic masses. A diagnostic mammogram is often performed in combination with a breast ultrasound in these patients for superior visualization of the area of concern (RadiologyInfo.org, 2019).

Ultrasound is a safe, noninvasive imaging modality that uses sound waves to generate images of internal body structures and carries no radiation exposure (Radiologyinfo.org, 2018). Magnetic resonance imaging (MRI) of the breast is particularly useful in women with dense or fibrotic breasts as it is superior in identifying abnormalities in soft tissues. It may also be used in specific circumstances, such as for patients with a prior history of breast cancer, to evaluate for contralateral disease, or for surgical planning. MRIs are distinct from other forms of diagnostic imaging as they do not use x-rays or pose radiation exposure. MRIs utilize strong electromagnetic fields and radio waves to measure how much water is within different tissues within the body and generate detailed images of the underlying tissues (US Food & Drug Administration [FDA], 2018d).
Tissue Sampling
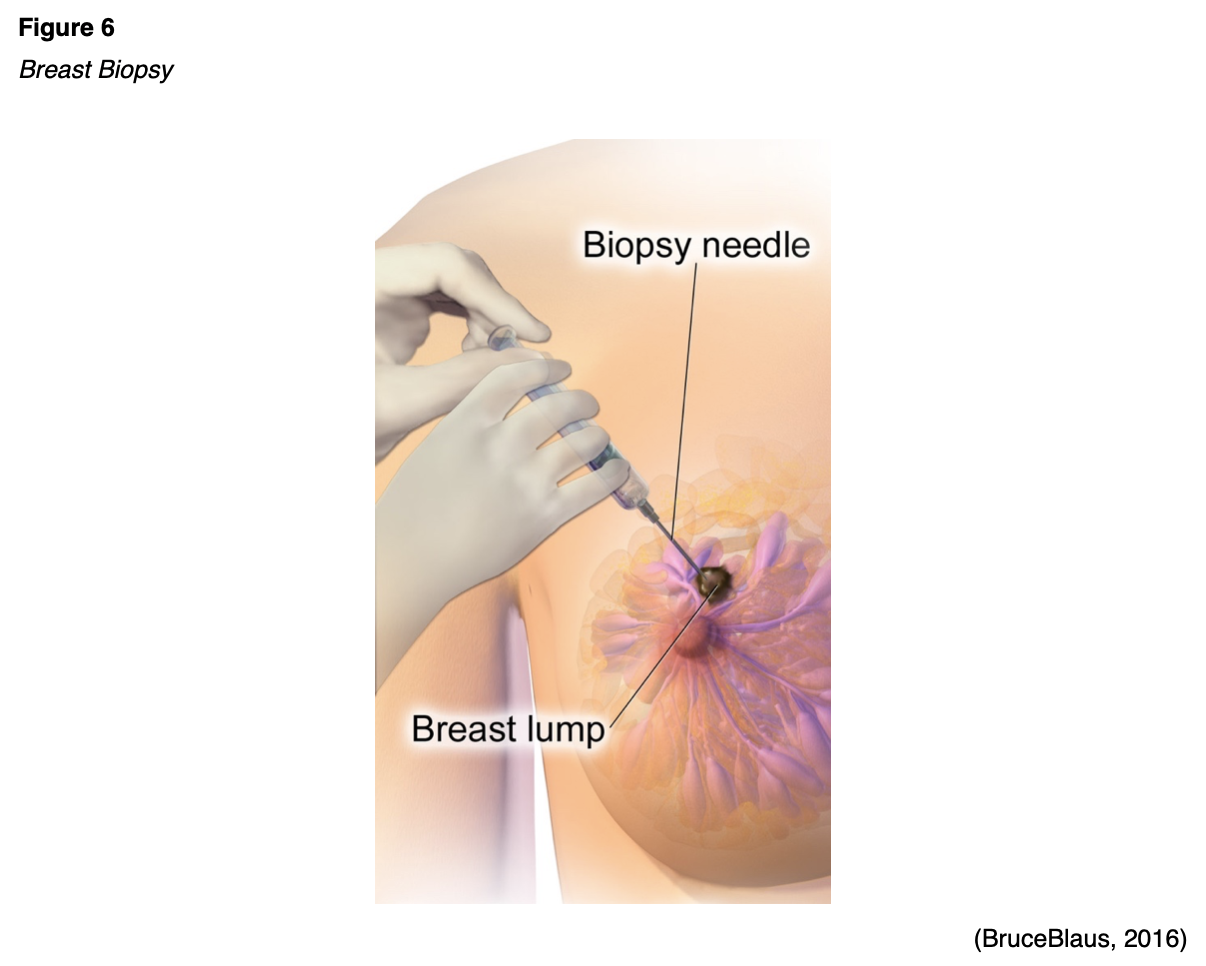
The only way to definitively confirm cancerous cells and establish the specific clinical features of the tumor is through tissue sampling, usually in the form of a breast biopsy, as demonstrated in Figure 6. The tissue cells or fluid are then examined under a microscope by a pathologist (National Breast Cancer Foundation, 2019a). The main types of breast biopsies include core needle biopsy, surgical biopsy or excision, and fine-needle aspiration (FNA). While FNA is a lower cost and minimally invasive procedure, it is substantially less accurate than the other two modalities and often requires a second diagnostic procedure. The preferred method is an image-guided core needle biopsy, which is associated with the highest diagnostic yield with minimal morbidity. It allows for the pertinent histologic evaluation testing to be performed on the tissue. If a core needle biopsy is not feasible or is non-diagnostic, only then should clinicians consider proceeding with a surgical biopsy or excision (Yarbro et al., 2018).
Breast Cancer Staging
The American Joint Committee on Cancer (AJCC) directs breast cancer staging, which has evolved over the years. As demonstrated in Figure 7, the stage of cancer depicts the extent of cancer growth and spread within the body. It is a core element when developing the most optimal, evidence-based treatment regimen, as breast cancer prognosis and treatment decisions are predicated on cancer staging and its specific clinical features. The most updated AJCC cancer staging (8th edition) includes all of the clinical features listed in Table 2, all of which can be evaluated using the biopsy tissue (Breastcancer.org, 2020a).



Treatment for breast cancer is typically multifactorial and involves the use of combined modalities. The vast majority of National Cancer Institute (NCI)-accredited institutions rely on the National Comprehensive Cancer Network (NCCN) evidence-based guidelines that outline treatments based on clinical features and staging. The NCCN (2020) is an alliance of leading cancer centers and world-renowned experts devoted to cancer care, research, and education. Through rigorous clinical trial research, data compiled across institutions, and annual expert panel reviews, the NCCN provides evidence-based treatment guidelines for cancer according to cancer type, pathology, genetics, staging, inheritance patterns, as well as several other specific features. The guidelines are widely utilized in cancer care and guide medical decision making throughout the patient’s disease trajectory (NCCN, 2020).
Surgery
Many patients will undergo surgery for breast cancer. The surgical options depend on the clinical features, size, extent, and stage of the tumor.
- Lumpectomy: the portion of the breast that contains the cancerous cells is excised while leaving the remainder of the healthy breast tissue is left in place.
- Axillary lymph node dissection (ALND): removal of affected lymph nodes in the axillary region; the amount removed depends on the extent of the cancer spread.
- Mastectomy:
- Total (simple) mastectomy: the breast tissue, nipple, areola, and skin are removed, but not all the lymph nodes. This procedure is demonstrated in Figure 8.
- Modified radical mastectomy: the entire breast and most of the axillary region and lymph nodes are removed, but the chest wall muscles under the breast remain.
- Radical mastectomy: the most extensive type of mastectomy in which the entire breast is removed, ALND, as well as the chest wall muscles under the breast.
- Partial mastectomy: the cancerous portion of the breast tissue is removed, along with some of the surrounding healthy tissue; this is very similar to lumpectomy, except more tissue is removed.
- Nipple-sparing mastectomy: all of the breast tissue is removed, except the nipple is spared.
- Prophylactic mastectomy: women with an increased risk for breast cancer due to BRCA1/2 genetic mutations or strong family history may consider bilateral prophylactic mastectomy as a risk reduction measure. Further, some women who have had cancer in one breast may also opt to have the other breast removed as a means of prevention (Breastcancer.org, 2020a).

Chemotherapy
Surgery for breast cancer may or may not be preceded by neoadjuvant chemotherapy or followed by adjuvant therapy. Neoadjuvant chemotherapy is administered to shrink a tumor so that the surgical intervention may not need to be as extensive. In breast cancer patients, neoadjuvant chemotherapy may shrink the tumor enough so that the breast surgeon may be able to perform a lumpectomy instead of a mastectomy. Adjuvant therapy is given following surgery to eradicate any micro-metastases. Micro-metastases are a small collection of cancer cells too tiny to be identified on imaging scans that have detached from the original tumor and spread to other parts of the body. The danger with micro-metastases is that they can group together and form additional cancerous tumors within the body. Adjuvant therapy aims to prevent cancer recurrence (Yarbro et al., 2018). Chemotherapy, also referred to as cytotoxic or antineoplastic therapy, encompasses a group of high-risk, hazardous drugs with the intent to destroy as many cancer cells with as minimal effect on healthy cells as possible. Premised on the concepts of cellular kinetics, chemotherapy generally works by interfering with the normal cell cycle, impairing DNA synthesis and cell replication, preventing cancer cells from dividing, multiplying, and forming into new cancer cells (Nettina, 2019). There is a wide range of chemotherapeutic agents used in breast cancer, and they are usually given in combinations of two or three drugs. The drug selection depends on the stage of breast cancer, and if the intent of treatment is curative or palliative. The most commonly used agents are as follows:
- Taxanes, such as paclitaxel (Taxol), docetaxel (Taxotere), and albumin-bound paclitaxel (Abraxane).
- Anthracyclines or antitumor antibiotics such as doxorubicin (Adriamycin) and epirubicin (Ellence).
- Antimetabolites such as 5-fluorouracil (5-FU), capecitabine (Xeloda), and gemcitabine (Gemzar).
- Alkylating agents such as cyclophosphamide (Cytoxan) and carboplatin (Paraplatin) (NCCN, 2020; Olsen et al., 2019).
The majority of chemotherapeutic agents are broad in their attack, meaning they kill normal, healthy cells in the body together with the cancer cells. As a result, they pose a wide array of several side effects, which can also vary based on the specific agent (Itano, 2016). For a detailed review of chemotherapy agents, their side effects, prescribing indications, and monitoring, refer to the “Oncology Prescribing” NursingCE course.
Radiation Therapy
Radiation therapy is a localized treatment that uses ionizing radiation to treat cancerous tumors, with the primary objective of delivering a precisely measured dose of radiation to a defined tumor with as little injury as possible to surrounding healthy tissue. Radiation induces cellular damage to cancer cells, leading to biological changes in the DNA. This causes cells to die over days, weeks, and months, rendering them incapable of reproducing or spreading. All healthy cells and cancer cells are vulnerable to the effects of radiation and may be injured or destroyed. However, most healthy, non-cancerous cells can repair themselves and remain functional, whereas the cancerous cells are destroyed from the radiation (Yarbro et al., 2018). In breast cancer, radiation is generally performed following surgery to reduce the risk that cancer will return in the same breast, surrounding tissue, or lymph nodes. It may also be indicated for women following surgery if the tumor was large, if cancer cells were found in the lymph nodes, or if the surgical margins demonstrate signs of disease. Further, radiation therapy can also be used to control symptoms and for pain relief in patients with metastases in other parts of the body, such as the bones or the brain (ACS, 2019).
The two main types of radiation therapy used to treat breast cancer include external beam radiation therapy (EBRT) and brachytherapy. ERBT is the most common method used for breast cancer; it uses an external beam of radiation that is specifically focused on the targeted area. EBRT usually begins about three to four weeks after surgery. It is administered for only a few minutes at a time, five days a week, for a period of five to six weeks. Brachytherapy is a form of internal radiation that is delivered through an implantable device that is placed inside the breast. Brachytherapy delivers targeted radiation to the tumor bed (or the location where cancer initially grew). Brachytherapy is often administered in only a few short treatments. Breast radiation is generally well-tolerated. The acute effects are usually transient, occur during treatment, limited to the skin, and generally subside within two weeks of treatment cessation. Skincare is critical in patients undergoing radiation as up to 95% of patients receiving radiation therapy will experience some degree of skin reaction. Cumulative doses of radiation weaken the skin integrity, depleting stem cells from the basal layer of the epidermis, leading to varying degrees of radiodermatitis. Skin reactions generally begin around 7-14 days after the initiation of treatment, and the first signs include dryness and erythema. These symptoms may progress to bright red erythema, rash, and desquamation (sloughing off of the top layer of the skin). Many patients describe that the skin feels similar to a sunburn. Additional effects of breast radiation include fatigue and an increased risk for lymphedema (Nettina, 2019; Yarbro et al., 2018).
Hormonal Therapy
Hormonal treatments are targeted agents that work by blocking the hormones from reaching the cancer cells or by preventing the body from producing the hormones (Nettina, 2019). Estrogen and estrogen receptors are key drivers in many breast cancers, thereby making them amenable to hormone-blocking treatments to shrink or slow their growth. In addition to being a viable treatment, hormonal therapy can also be administered as chemoprevention to lower the risk of ER/PR-positive breast cancer in individuals who are at high-risk but haven’t been diagnosed with breast cancer. Tamoxifen (Soltamax) is the oldest hormonal treatment for breast cancer, initially approved by the FDA in 1977. It is an estrogen agonist/antagonist approved for the treatment of HR-positive breast cancers as well as a risk-reducing agent in patients with DCIS. Further, tamoxifen (Soltamax) is the most common agent used for chemoprevention in high-risk patients. The recommended duration of treatment is 5 to 10 years (FDA, 2018c). Currently, there are four major types of hormonal therapy, which include selective estrogen receptor modulators (SERM), selective estrogen receptor down-regulators (SERD), luteinizing hormone-releasing hormones (LHRH), and aromatase inhibitors (AI), which are outlined in Table 3. The most common adverse effects of hormone treatment depend on the type of drug and can differ between men and women, but generally include hot flashes, night sweats, loss of libido, weight gain, joint aches or pains, mood changes, thinning or weakening of the bones (osteopenia or osteoporosis), and atrophic vaginitis (atrophy, loss of elasticity, dryness, and resulting irritation of the vaginal mucosa). Men who take hormonal therapy for breast cancer may experience hot flashes, erectile dysfunction, shrinking of the testicles, and gynecomastia (enlargement of breast tissue). Due to the impact of hormonal therapy on bone thinning, patients should be counseled on the importance of a calcium-rich diet with at least 1,200 mg of dietary calcium daily. Patients who are unable to get this recommended amount of calcium in their diet should consider calcium supplementation. Clinicians should also counsel patients on the importance of engaging in weight-bearing exercises for bone health. Exercise can also help reduce the severity of joint aches and pains associated with these medications (Olsen et al., 2019)
Table 3
Hormonal Treatments for Breast Cancer
Drug & Dosing | Indications & Mechanism | Warnings & Precautions |
SERM
- Tamoxifen (Soltamax) 20 mg po daily
| - Oral agents generally indicated for premenopausal women.
- Partial agonist that blocks estrogen receptors or breast cancer cells.
| - Increased risk of uterine malignancies; counsel patients to promptly report abnormal vaginal bleeding.
- Increased risk for thromboembolic events, such as stroke, deep vein thrombosis (DVT), and pulmonary embolism (PE).
|
SERD
- Fulvestrant (Faslodex) 500 mg IM injection on days 1, 15, 29, and then once monthly thereafter.
| - It is indicated for postmenopausal women not previously treated with endocrine therapy or with disease progression after endocrine therapy and in combination with an oral CDK 4/6 inhibitor.
- Binds to estrogen receptor and downregulates estrogen in breast cancer cells.
- It blocks estrogen throughout the body.
| - Injection site reactions.
- Elevated hepatic enzymes.
- Embryo-Fetal Toxicity.
|
LHRH
- Leuprolide acetate (Lupron) 7.5 mg IM injection once monthly, or 22.5 mg IM once every three months
| - It is used to reduce the risk of early-stage breast cancer from recurring in premenopausal women.
- Blocks the signals to the ovaries and stops them from generating estrogen; induces chemical menopause, so there is less estrogen to fuel the growth of cancer.
- It is commonly used in conjunction with an AI in premenopausal women.
| - Hyperglycemia and increased risk of diabetes.
- Increased risk of myocardial infarction, sudden cardiac death, and stroke.
- May prolong the QTc interval.
- Once the LHRH is discontinued, the ovaries usually recover and resume normal functioning over time.
|
AI
- Anastrozole (Arimidex) 1 mg po daily
- Letrozole (Femara) 2.5 mg po daily
- Exemestane (Aromasin) 25 mg po daily
| - Since estrogens are mostly derived from the action of the aromatase enzyme in postmenopausal women, anastrozole (Arimidex) and letrozole (Femara) are selective nonsteroidal agents that bind to and inhibit the aromatase enzyme.
- Exemestane (Aromasin) is a steroidal aromatase inactivator that binds irreversibly to the aromatase enzyme, inactivating it.
- AIs are oral agents indicated for postmenopausal women, as they are considered much more effective than tamoxifen (Soltamax) within postmenopausal women.
- It is also indicated for use in postmenopausal women with disease progression while on tamoxifen (Soltamax).
| - Does not carry a risk for uterine malignancies or thromboembolic events.
- Increased risk for osteoporosis, cardiac effects, and debilitating joint stiffness or joint pain.
|
(AbbVie Inc., 2019; ANI Pharmaceuticals, Inc., 2019; Breastcancer.org, 2016; FDA, 2017, 2018c)
Targeted Therapies
Targeted therapies refer to a few classes of novel treatment modalities that function by attacking specific parts of cancer cells to prevent tumor development or to shrink existing tumors. There are numerous proteins located on the cellular membranes called growth factor receptors, which connect the external and internal cellular environments and are essential for cell growth and development. These drugs can block or turn off chemical signals that tell the cancer cell to grow and divide, starve the tumor by cutting off blood supply and/or by preventing the formation of new blood vessels, or carry toxins or poison directly to the cancer cells, killing them without harming healthy cells (Sengupta, 2017). The development of specialized drugs that block these growth factor receptors has been a tremendous part of breast cancer research throughout the last few decades. These drugs have revolutionized treatment options for patients living with advanced and metastatic breast cancer by fighting against drug resistance and increasing survival. The next section provides an overview of the major classes and types of targeted oral agents used to treat breast cancer (Breastcancer.org, 2020b; Masoud & Pages, 2017; NCCN, 2020).
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors
CDK4/6 inhibitors work by interrupting intracellular pathways and hormone signals that have roles in stimulating the growth and proliferation of cancerous cells (Scott et al., 2017). They are all slightly different, but the basic concept is that CDK4/6 pathways are key drivers in HR-positive, HER2/neu-negative metastatic breast cancer. There are currently three CKD4/6 inhibitors approved by the FDA for use in combination with an aromatase inhibitor or fulvestrant (Faslodex) for women with HR-positive, HER2/neu-negative advanced or metastatic breast cancer, which include palbociclib (Ibrance), abemaciclib (Verzenio), and ribociclib (Kisquali). These drugs have not been directly compared yet are considered equivalent in efficacy (Shah et al., 2018).
- Palbociclib (Ibrance) 125 mg po daily for three weeks on, followed by one week off.
- Ribociclib (Kisqali) 600 mg po daily for three weeks on, followed by one week off.
- Abemaciclib (Verzenio) 150 mg po twice daily in combination with fulvestrant (Faslodex), or 200 mg po twice daily as monotherapy.
Oral CDK4/6 inhibitors are generally well tolerated. As a class, the most common adverse effects include bone marrow suppression (neutropenia, anemia, and thrombocytopenia), diarrhea, and fatigue. CDK4/6 inhibitors are associated with a low risk (~1.1%) of interstitial lung disease (ILD)/pneumonitis. Neutropenia is the most common adverse effect of ribociclib (Kisqali) and palbociclib (Ibrance), requiring close monitoring of blood counts. If significant neutropenia develops, dose interruption and/or dose reduction may be necessary. Ribociclib (Kisqali) has the highest affinity for CDK4 when compared with the other CDK4/6 inhibitors. Therefore, it carries additional risks, including hepatobiliary toxicity and QTc interval prolongation; it requires monitoring of hepatic function tests and serial ECGs at defined intervals and as clinically indicated. Diarrhea is the most common side effect of abemaciclib (Verzenio), affecting 85% to 90% of patients (Shah et al., 2018).
Phosphatidylinositol-3-kinase (PI3K) Inhibitor
Mutations in the PIK3CA gene in HR-positive and HER2/neu-negative breast cancers are a common cause of cancer growth and resistance to hormonal treatments over time. Worldwide, nearly 40% of HR-positive, HER2/neu-negative breast cancer patients have a PIK3CA mutation. Alpelisib (Piqray) works by inhibiting PI3K, which induces an increase in estrogen receptor transcription in breast cancer cells. When combined with fulvestrant (Faslodex), it has demonstrated increased antitumor activity among patients that harbor the PIK3CA mutation. Alpelisib (Piqray) is FDA-approved only in conjunction with fulvestrant (Faslodex) in postmenopausal women (and men) with HR-positive, HER2/neu-negative, PIK3CA-mutated advanced or metastatic breast cancer. It is dosed at 300 mg po once daily with fulvestrant (Faslodex) 500 mg IM injection on days 1, 15, 29, followed by once monthly thereafter (FDA, 2019b). In the SOLAR-1 trial, a double-blind, placebo-controlled multicenter phase 3 study in men and postmenopausal women with PIK3CA mutations, alpelisib (Piqray) nearly doubled progression-free survival (11.0 months versus 5.7 months in the placebo group; Andre et al., 2019). The most common side effects include diarrhea, nausea, fatigue, anorexia, and skin rash. The drug is also associated with severe adverse reactions, including hypersensitivity requiring drug discontinuation, severe skin reactions, hyperglycemia, and diarrhea. Patients require close monitoring of fasting blood glucose (FBG) and hemoglobin A1C (HbA1C), as there are strict guidelines for managing hyperglycemia while on this medication. Patients may require dose interruption, dose reduction, as well as the initiation of oral antihyperglycemics such as metformin (Glucophage) to optimize glucose control. Further, the cutaneous reactions can be severe, requiring close monitoring, dose modifications, and intervention with topical steroids. In severe cases, the drug may also need to be discontinued permanently (Andre et al., 2019; FDA, 2019b).
Mammalian Target of Rapamycin (mTOR) Pathway
The mTOR pathway is part of a complex intracellular pathway that serves as a key regulator of cell physiology in various types of cancers. It is used as a drug target in several types of cancers due to its links to various cellular and physiological functions involved in cellular growth, proliferation, and survival. Everolimus (Afinitor) is an mTOR inhibitor approved for use in postmenopausal women with HR-positive, HER2/neu-negative, advanced breast cancer in combination with exemestane (Aromasin) following a prior failure of treatment with letrozole (Femara) or anastrozole (Arimidex). Everolimus (Afinitor) is dosed at 10 mg once daily, and the most common side effect is oral mucositis, which is inflammation, irritation, and swelling of the oral mucosa and lips, which can lead to painful ulcers that can develop within two weeks of starting the medication. Patients should be educated on routine oral hygiene practices to maintain the integrity of the oral mucosa, such as using soft-bristled toothbrushes and avoiding alcohol-based mouthwashes as well as hot foods or those that can cause oral irritation and dryness. Additional reported side effects include fatigue, anorexia, skin rash, diarrhea, and increased serum cholesterol levels. It carries a risk for pneumonitis, impaired wound healing, renal failure, and embryo-fetal toxicity. Everolimus (Afinitor) is also associated with potential increased risk for angioedema in patients taking concomitant angiotensin-converting enzyme (ACE) inhibitors (FDA, 2018a).
Poly ADP-ribose Polymerase (PARP) Inhibitors
The PARP enzyme has a critical role in cell growth, regulation, and repair of both healthy cells and cancer cells. In cancer cells, it fixes DNA damage, essentially helping cancer cells repair themselves and survive (Olsen et al., 2019). PARP inhibitors interfere with the PARP enzyme, making it more difficult for cancer cells with a BRCA1 or BRCA2 mutation to repair DNA damage, thereby inducing cell death. PARP-inhibitors have transformed the treatment of BRCA–mutation positive cancers, such as ovarian cancer and breast cancers (Ring & Modesitt, 2018). Olaparib (Lynparza) is FDA-approved to treat metastatic HER2/neu-negative breast cancer with an inherited BRCA1 or BRCA2 mutation that has previously been treated with chemotherapy. Olaparib (Lynparza) is administered at a dose of 300 mg po twice daily. The most common side effects include anemia, neutropenia, fatigue, nausea, diarrhea or constipation, anorexia, and arthralgias. Olaparib (Lynparza) is also associated with a rare risk (less than 1.5%) of developing myelodysplastic syndrome (MDS), a bone marrow failure disorder, or acute myeloid leukemia (AML), a type of blood cancer. It is also associated with a slight risk (less than 1%) of pneumonitis and embryo-fetal toxicity. PARP inhibitors have several important drug interactions, particularly antifungal medications and certain antibiotics. Patients should be counseled to alert their clinician prior to starting any new medications. In addition, patients should avoid grapefruit and Seville oranges, which can increase the effects of PARP-inhibitors and lead to toxicity. Clinical research continues to explore PARP inhibitors’ effectiveness in additional settings (FDA, 2018b; NCCN, 2020).
Monoclonal antibodies
Monoclonal antibodies are a type of targeted therapy that function by locating and attaching to specific receptors on the surface of cancer cells, such as the HER2/neu receptor. HER2/neu-positive breast cancer is amenable to HER2 directed monoclonal antibody treatments, such as trastuzumab (Herceptin) or pertuzumab (Perjeta). These agents are recombinant DNA-derived humanized monoclonal antibodies that selectively bind with high affinity in a cell-based assay to the extracellular domain of the HER2/neu receptor, inducing cell death. They are approved for treating patients with early-stage and advanced metastatic breast cancer whose tumors overexpress HER2/neu (Olsen et al., 2019). Trastuzumab (Herceptin) was the first drug approved by the FDA in 1998 for the treatment of HER2/neu-positive breast cancer. Trastuzumab (Herceptin) and pertuzumab (Perjeta) are intravenous infusions that may be used together, as well as in combination with certain chemotherapy agents. In women who are being treated with curative intent, these medications are given for 12-months; however, they may also be used in advanced and metastatic settings indefinitely as tolerated. Both drugs carry boxed warnings for cardiotoxicity, as they can lead to cardiac failure manifesting as decreased left ventricular dysfunction (LVEF) or congestive heart failure (CHF). Clinicians are advised to evaluate pre-treatment cardiac studies (i.e., echocardiogram or multiple-gated acquisition [MUGA] scan) to establish a baseline, followed by serial LVEF evaluations at defined intervals during treatment, and then every six months up to two years following the completion of treatment. There are specific guidelines for discontinuing or delaying treatment in the event of a confirmed clinically significant decline in LVEF. In addition, these agents carry another boxed warning for embryo-fetal toxicity, as exposure can result in embryo-fetal death and birth defects. Diarrhea is a common side effect of pertuzumab (Perjeta), with the incidence ranging from 28% to 72%. Clinical studies demonstrate the incidence is highest during the first treatment, decreasing with subsequent cycles. Despite the high incidence of diarrhea in patients on pertuzumab (Perjeta), research demonstrates that it can usually be managed effectively without causing severe toxicity, treatment delays, or drug discontinuation (Swain et al., 2017).
Researchers continue to study the HER2/neu gene extensively. One of the most recent treatment developments is trastuzumab emtansine (Kadcyla), also called T-DMI. This is an antibody-drug conjugate of trastuzumab (Herceptin) that is linked to a cytotoxic agent. A conjugate is a compound that is combined with a chemotherapeutic agent as a means to induce a greater cell kill. Based on the KATHERINE trial, the risk of recurrence of invasive breast cancer or death was 50% lower with T-DM1 than with trastuzumab (Herceptin) alone. Due to these promising results, trastuzumab emtansine (Kadcyla) was approved by the FDA in 2019 for the treatment of early-stage, HER2/neu-positive breast cancer with residual disease after surgery, for initial adjuvant treatment, and metastatic breast cancer (Minckwitz et al., 2019). Trastuzumab emtansine (Kadcyla) is administered as an intravenous infusion every three weeks for 14 doses. It carries a boxed warning for hepatotoxicity, liver failure, and death. Clinicians must monitor the patient’s hepatic function prior to each dose, as some patients require dosing modifications or permanent discontinuation. It also carries the same boxed warnings as trastuzumab (Herceptin), which include cardiotoxicity requiring serial monitoring of LVEF and risk for embryo-fetal toxicity. While trastuzumab emtansine (Kadcyla) is generally well tolerated, the most common adverse reactions include fatigue, nausea, musculoskeletal pain, hemorrhage, thrombocytopenia, headache, increased transaminases, constipation, epistaxis, and arthralgias (FDA, 2019a).
Learn much more about these cancer treatment modalities, side effects, monitoring parameters, and nursing considerations with our Oncology Nursing CE courses and earn up to 10 ANCC credits.
The Early Detection of Breast Cancer
Breast Cancer Risk Assessment: Gail Model
Cancer risk assessment tools help estimate the risk for specific cancer types, guide evidence-based interventions to reduce that risk, and are intended for use as an adjunct to an individualized, comprehensive cancer risk assessment. The Gail Model is the most commonly used breast cancer risk assessment tool to estimate a woman’s five-year risk and overall lifetime risk for developing breast cancer (Smith et al., 2019). There are limitations to this tool, as it cannot calculate the risk in women under the age of 35, those with inherited mutations in BRCA1/2, or women with a history of invasive or in situ breast cancers. The tool is available online via the NCI (n.d.) at bcrisktool.cancer.gov.
Breast Cancer Screening
Screening tests are performed to diagnose cancer before it grows large enough to cause symptoms and is still treatable or potentially curable. Early detection refers to finding and diagnosing the disease earlier than if the individual waited for the symptoms to develop. Breast cancers identified during screening exams are more likely to be small and still confined to the breast. The size of the tumor and whether or not it has spread are some of the most critical factors in predicting the patient’s prognosis, as tumor size at the time of diagnosis is directly related to mortality. Breast cancer screening is most commonly performed through mammography. Screening mammography beginning at age 40 saves the most lives and saves the most years of life, and annual screening saves more lives than every other year (biennial) (ACS, 2020a). Annual mammography screening in premenopausal women is associated with a significantly decreased risk of identifying advanced breast cancer than screening performed every other year. Postmenopausal women do not receive the same benefits of annual screening unless they are currently receiving hormone replacement therapy (HRT) for menopause; therefore, women 55 years or older can undergo screening every other year. The age to discontinue screening is not yet definitively established. Research demonstrates that continued screening may be beneficial in certain women 75 years or older, depending on their mortality risk, comorbidities, overall health, and performance status (CDC, 2018b). All women should be familiar with the known benefits, limitations, and potential harms of breast cancer screening. Women should check their breasts regularly to know how their breasts typically look and feel and report any breast changes to their healthcare provider immediately (ACS, 2020a; Smith et al., 2019).
Average-Risk Women
The current ACS (2020a) recommendations for screening practices among average-risk women include the following:
- Women aged 40 to 44 should have the opportunity to begin annual screening with mammography.
- In women aged 45 to 54, annual mammography should be routinely performed.
- Women aged 55 or older should transition to biennial screening (screening every two years) or may continue screening annually.
- Women should continue screening mammography as long as their overall health is good, and they have a life expectancy of 10 years or longer (ACS, 2020a; Smith et al., 2019).
High-Risk Women
Women who are known or likely carriers of the BRCA1/BRCA2 gene mutations and other high‐risk genetic syndromes or who have been treated with radiation to the chest for Hodgkin disease or other cancers are considered at increased risk. Annual screening mammography and MRI starting at age 30 are recommended for women who meet any of the following criteria:
- Have a known BRCA1 or BRCA2 gene mutation.
- Are untested but have a first‐degree relative with a BRCA mutation.
- Have a 20% to 25% or higher lifetime risk of breast cancer based upon specialized breast cancer risk‐estimation models capable of pedigree analysis of first‐degree and second‐degree relatives on both the maternal and paternal sides.
- Women who were treated for Hodgkin disease with radiation to the chest wall between the ages of 10 and 30 years (ACS, 2020a; Smith et al., 2019).
Cancer Survivorship and the Fundamental Role of Primary Care APRNs
According to the NCI Office of Cancer Survivorship (2020), “an individual is considered a cancer survivor from the time of diagnosis, through the balance of his or her life. There are many types of survivors, including those living with cancer and those free of cancer.” As of January 2019, there are an estimated 16.9 million cancer survivors in the US, representing approximately 5% of the population. Of these, 3.9 million (23%) are breast cancer survivors, and these numbers are both projected to rise over the next decade due to continued developments in research and technology (Miller et al., 2019; NCI Office of Cancer Survivorship, 2020). Cancer survivors have unique physical, emotional, and psychosocial needs that require oversight of a skilled and knowledgeable healthcare team. APRNs practicing in primary care serve pivotal roles in the early detection of cancer, managing survivors’ unique physical and psychosocial needs, and coordinating care throughout the cancer survivorship period. Primary care APRNs are tasked with addressing and mitigating negative health behaviors associated with cancer, administering cancer-preventing vaccinations, and are the main drivers of screening and early detection practices for cancer. They are uniquely positioned to address the needs of survivors to improve the quality of life and preserve health and well-being. Therefore, primary care APRNs are tasked with acquiring the skillset to identify abnormal signs of cancer early, manage the late effects of cancer-related treatment, and recognize the signs of cancer recurrence to facilitate timely intervention. They support cancer survivors as they reintegrate into society following cancer treatment, which is often accompanied by significant changes in lifestyle, family dynamics, and poses new health concerns, including heightened screening and surveillance. APRNs serve fundamental roles in patient education and improving the quality and longevity of life throughout cancer survivorship (Nettina, 2019).
Learn more about cancer prevention, early detection, and cancer survivorship with our NursingCE courses: Cancer Prevention and Early Detection (4 ANCC credits) and Cancer Survivorship (2 ANCC credits).
References
AbbVie Inc. (2019). Lupron depot® (leuprolide acetate for depot suspension). http://www.lupron.com/
American Cancer Society. (2019). Radiation for breast cancer. https://www.cancer.org/cancer/breast-cancer/treatment/radiation-for-breast-cancer.html
American Cancer Society. (2020a). American cancer society recommendations for the early detection of breast cancer. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
American Cancer Society. (2020b). Cancer facts & figures, 2020. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf
American Cancer Society. (2020c). Survival rates for breast cancer. https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-survival-rates.html
American College of Obstetricians and Gynecologists. (2017). Breast cancer risk assessment and screening in average-risk women. ACOG Practice Bulletin, 179, 1-16. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women.pdf
Andre, F., Ciruelos, E., Rubovszky, G., Compone, M., Loibl, S., Rugo, H. S., Iwata, H., Conte, P., Mayer, I. A., Kaufman, B., Yamashita, T., Lu, Y., Inoue, K., Takahashi, M., Papai, Z., Longin, A., Mills, D., Wilke, C., Hirawat, S., … SOLAR-1 Study Group. (2019). Alpelisib for PIK3CA-mutated, hormone-receptor-positive advanced breast cancer. New England Journal of Medicine, 380(20), 1929-1940. https://doi.org/10.1056/NEJMoa1813904
ANI Pharmaceuticals, Inc. (2019). Important safety information about Arimidex. https://www.arimidex.com/
Breastcancer.org. (2016). Lupron. https://www.breastcancer.org/treatment/druglist/lupron
Breastcancer.org. (2020a). Breast cancer stages. https://www.breastcancer.org/symptoms/diagnosis/staging
Breastcancer.org. (2020b). Targeted therapies. https://www.breastcancer.org/treatment/targeted_therapies
Breastcancer.org. (2020c). US breast cancer statistics. https://www.breastcancer.org/symptoms/understand_bc/statistics
BruceBlaus. (2014). Mammography [image]. https://commons.wikimedia.org/wiki/File:Blausen_0628_Mammogram.png
BruceBlaus. (2016). Breast biopsy [image]. https://commons.wikimedia.org/wiki/File:Needle_Breast_Biopsy.png
The Centers for Disease Control and Prevention. (2018a). What are the risk factors for breast cancer? https://www.cdc.gov/cancer/breast/basic_info/risk_factors.htm
The Centers for Disease Control and Prevention. (2018b). What is breast cancer screening? https://www.cdc.gov/cancer/breast/basic_info/screening.htm
The Centers for Disease Control and Prevention. (2019a). BRCA gene mutations. https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/brca_gene_mutations.htm
The Centers for Disease Control and Prevention. (2019b). Jewish women and BRCA gene mutations. https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/jewish_women_brca.htm
The Centers for Disease Control and Prevention. (2020). Breast cancer statistics. https://www.cdc.gov/cancer/breast/statistics/index.htm
Domaina. (2012). Autosomal dominant [image]. https://commons.wikimedia.org/wiki/File:Autosomal_dominant_-_en.svg
Koh, J., & Kim, M. J. (2019). Introduction of a new staging system of breast cancer for radiologists: An emphasis on the prognostic stage. Korean Journal of Radiology, 20(1), 69-82. https://doi.org/10.3348/kjr.2018.0231
Masoud, V., & Pages, G. (2017). Targeted therapies in breast cancer: New challenges to fight against resistance. World Journal of Clinical Oncology, 8(2), 120-134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5385433/
McCance, K. L., & Heuther, S. E. (2019). Pathophysiology: The biologic basis for disease in adults and children. (8th ed.). Elsevier.
Miller, K. D., Nogueria, L., Mariotto, A. B., Rowland, J. H., Yarbroff, R., Alfano, C. M., Jemal, A., Kramer, J. L., & Siegel, R. L. (2019). Cancer treatment and survivorship statistics, 2019. CA: A Cancer Journal for Clinicians, 69(5), 363-385. https://doi.org/10.3322/caac.21565
Minckwitz, G., Huang, C., Mano, M., Loibl, S., Mamounas, E., Untch, M., Wolmark, N., Rastogi, P., Schneeweiss, A., Redondo, A., Fischer, H., Jacot, W., Conlin, A., Arce-Salinas, C., Wapnir, I., Jackisch, C., DiGiovanna, M., Fasching, P., Crown, J., … Geyer, C. (2019). Trastuzumab emtansine for residual invasive HER2-positive breast cancer. New England Journal of Medicine, 380(7),617-628. https://doi.org/10.1056/NEJMoa1814017
National Breast Cancer Foundation. (2019a). Diagnosis. https://www.nationalbreastcancer.org/breast-cancer-diagnosis/
National Breast Cancer Foundation. (2019b). Types of breast cancer. https://www.nationalbreastcancer.org/types-of-breast-cancer/
National Cancer Institute. (n.d.). The breast cancer risk assessment tool. Retrieved August 15, 2020, from https://bcrisktool.cancer.gov/index.html
National Cancer Institute. (2012). Total (simple) mastectomy [image].
https://commons.wikimedia.org/wiki/File:Total_(simple)_mastectomy.jpg
National Cancer Institute Office of Cancer Survivorship. (2020). Statistics, graphs, and definitions. https://cancercontrol.cancer.gov/ocs/statistics/index.html#definitions
National Comprehensive Cancer Network. (2020). NCCN clinical practice guidelines in oncology (NCCN Guidelines®) breast cancer version 5.2020 - July 15, 2020. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf
Nettina, S. M. (2019). Lippincott manual of nursing practice (11th ed.). Wolters Kluwer.
OncotypeIQ. (2020). About the oncotype DX breast recurrence score® test. https://www.oncotypeiq.com/en-US/breast-cancer/healthcare-professionals/oncotype-dx-breast-recurrence-score/about-the-test
Olsen, M., LeFebvre, K., & Brassil, K. (2019). Chemotherapy and immunotherapy guidelines and recommendations for practice. (1st Ed.). Oncology Nursing Society.
RadiologyInfo.org. (2018). General ultrasound.
https://www.radiologyinfo.org/en/info.cfm?pg=genus
RadiologyInfo.org. (2019). Mammography.
https://www.radiologyinfo.org/en/info.cfm?pg=mammo
Raphseck. (2016). Breast cancer warning signs [image]. https://commons.wikimedia.org/wiki/File:Breast_cancer_illustration_en.svg
Ring, K. L., & Modesitt, S. C. (2018). Hereditary cancers in gynecology. Obstetrics and Gynecology Clinics, 45(1), 155-173. https://doi.org/10.1016/j.ogc.2017.10.011
Scott, S. C., Lee, S. S., & Abraham, J. (2017). Mechanisms of therapeutic CDK4/6 inhibition of breast cancer. Seminars in Oncology, 44(6), 385-394. https://doi.org/10.1053/j.seminoncol.2018.01.006
Sengupta, S. (2017). Cancer nanomedicine: Lessons for immune-oncology. Trends Cancer, 3(8), 551-560. https://doi.org/10.1016/j.trecan.2017.06.006.
Shah, M., Nunes, M. R., & Stearns, V. (2018). CKD4.6 inhibitors: Game changes in the management of hormone-receptor-positive advanced breast cancer? Oncology (Williston Park), 32(5), 216-222. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6424488/pdf/nihms-1010845.pdf
Siegel, R. L., Miller, K. D., & Jemal, A. (2017). Cancer statistics, 2017. CA Cancer Journal for Clinicians, 67(1), 7-30. https://doi.org/10.3322/caac.21387
Simplyanon. (2011). Cancer staging [image]. https://en.m.wikipedia.org/wiki/File:Cancer_stages.png
Smith, R. A., Andrews, K. S., Brooks, D., Fedewa, S. A., Manassaram-Baptiste, D., Saslow, D., & Wender, R. C. (2019). Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA: A Cancer Journal for Clinicians, 69(3), 184-210. https://doi.org/10.3322/caac.21557
Swain, S. M., Schneeweiss, A., Gianni, L., Gao, J. J., Stein, A., Waldron-Lynch, M., Heeson, S., Beattie, M. S., Yoo, B., Cortes, J., & Baselga, J. (2017). Incidence and management of diarrhea in patients with HER2-positive breast cancer treated with pertuzumab. Annals of Oncology, 28(4), 761-768. https://doi.org/10.1093/annonc/mdw695
US Food & Drug Administration. (2017). Highlights of prescribing information: Faslodex® (fulvestrant). https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/021344s034lbl.pdf
US Food & Drug Administration. (2018a). Highlights of prescribing information: Afinitor®(everolimus). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022334s040,203985s013lbl.pdf
US Food & Drug Administration. (2018b). Highlights of prescribing information: Lynparza® (olaparib). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208558s001lbl.pdf
US Food & Drug Administration. (2018c). Highlights of prescribing information: Soltamox® (tamoxifen citrate). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021807s005lbl.pdf
US Food & Drug Administration. (2018d). MRI (magnetic resonance imaging). https://www.fda.gov/radiation-emitting-products/medical-imaging/mri-magnetic-resonance-imaging
US Food & Drug Administration. (2019a). Highlights of prescribing information: Kadcyla® (ado-trastuzumab emtansine). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/125427s105lbl.pdf
US Food & Drug Administration. (2019b). Highlights of prescribing information: PIQRAY® (alpelisib). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212526s000lbl.pdf
US National Library of Medicine. (2020). Breast cancer. https://ghr.nlm.nih.gov/condition/breast-cancer#sourcesforpage
Watkins, E. J. (2019). Overview of breast cancer. American Academy of Physician Assistants, 32(10), 13-17. https://doi.org/10.1097/01.JAA.0000580524.95733.3
Yarbro, C. H., Wujcik, D., & Gobel, B. H. (Eds.). (2018). Cancer nursing: Principles and practice. (8th ed.). Jones & Bartlett Learning.