This module aims to augment nursing knowledge of breast cancer by providing an overview of the condition, its risk factors, clinical features, common subtypes, treatment modalities, and the most common adverse effects of systemic therapies, as well as key patient teaching points.
...purchase below to continue the course
ain of lymph nodes (McCance & Heuther, 2019).
The pathophysiology of breast cancer is complex and multidimensional. Breast cancer is a heterogeneous disease with various molecular, genetic, and pathologic alterations. Breast cancer subtypes are classified by their specific clinical features, including histology, anatomical origin, tumor staging, hormone receptivity, and human epidermal growth factor receptor 2 (HER2) expression. The three most common types of receptors known to fuel most breast cancer growth include the estrogen receptor (ER), progesterone receptor (PR), and the HER2/neu gene expression. Awareness of the presence or absence of these receptors is vital to determining the most optimal, evidence-based treatment regimen. Overexpression of HER2/neu is associated with poorer overall survival rates, especially in patients who have lymph node metastasis (Masoud & Pages, 2017). The most common expression status of breast cancer is hormone-receptor (HR)-positive, HER2/neu-negative. While there are several types of breast cancer diagnoses, the major subtypes are explained in Table 1 (Watkins, 2019).



Signs and Symptoms
Early breast cancer generally has no signs or symptoms due to its small size and is most commonly identified on routine screening with mammography. If the breast tumor grows large enough, the most common signs include a unilateral, palpable mass with irregular borders. It may be a painless lump that is immobile or fixed to the skin and may or may not be accompanied by enlarged axillary lymph nodes. Some women may report changes to the breast caliber, texture, or shape, including asymmetry or open wounds or lesions that arise spontaneously. As demonstrated in Figure 3, skin changes such as retraction, thickening, or dimpling of the skin on the breast may also occur. Nipple changes may also occur, including retraction of the nipple or spontaneous discharge. Blood or purulent discharge expelled from the nipple is an ominous sign of underlying pathology (Nettina, 2019).

Diagnostic Imaging
Most breast cancers in the US are identified through mammography screenings. Mammography and ultrasonography are the most common breast imaging tests. As demonstrated in Figure 4, mammography uses low-dose x-rays to view inside the breast as a means to identify abnormalities suspicious for breast cancer. A standard mammogram is equivalent to approximately seven weeks of natural background radiation. In modern medicine, mammography is performed as a screening modality or as a diagnostic test. Diagnostic mammography differs from screening mammography in that it is supervised by a radiologist to tailor the additional views toward the area of suspicion to better characterize the abnormality, and a breast biopsy is commonly advised for highly suspicious findings (Koh & Kim, 2019).

Ultrasound is a safe, noninvasive imaging modality that uses sound waves to generate images of internal body structures and carries no radiation exposure (Radiologyinfo.org, 2018). Magnetic resonance imaging (MRI) of the breast is particularly useful in women with dense or fibrotic breasts as it is superior in identifying abnormalities in soft tissues. It may also be used in specific circumstances, such as for patients with a prior history of breast cancer, to evaluate for contralateral disease, or for surgical planning. MRIs utilize strong electromagnetic fields and radio waves to measure how much water is within different tissues within the body and generate detailed images of the underlying tissues (US Food & Drug Administration [FDA], 2018d).
Tissue Sampling
The only way to definitively confirm cancerous cells and establish the specific clinical features of the tumor is through tissue sampling, usually in the form of a breast biopsy, as demonstrated in Figure 5. The tissue cells or fluid are then examined under a microscope by a pathologist (National Breast Cancer Foundation, 2019a).

Breast Cancer Staging
The American Joint Committee on Cancer (AJCC) directs breast cancer staging, which has evolved over the years. As demonstrated in Figure 6, the stage of cancer depicts the extent of cancer growth and spread within the body. It is a core element when developing the most optimal, evidence-based treatment regimen, as breast cancer prognosis and treatment decisions are predicated on cancer staging and its specific clinical features. The most updated AJCC cancer staging (8th edition) includes all of the clinical features listed in Table 2, all of which can be evaluated using the biopsy tissue (Breastcancer.org, 2020a).


Treatment Modalities

Treatment for breast cancer is typically multifactorial and involves the use of combined modalities. The vast majority of National Cancer Institute (NCI)-accredited institutions rely on the National Comprehensive Cancer Network (NCCN) evidence-based guidelines that outline treatments based on clinical features and staging. The NCCN (2020) is an alliance of leading cancer centers and world-renowned experts devoted to cancer care, research, and education. Through rigorous clinical trial research, data compiled across institutions, and annual expert panel reviews, the NCCN provides evidence-based treatment guidelines for cancer according to cancer type, pathology, genetics, staging, inheritance patterns, as well as several other specific features. The guidelines are widely utilized in cancer care and guide medical decision making throughout the patient’s disease trajectory (NCCN, 2020).
Surgery
Many patients will undergo surgery for breast cancer. The surgical options depend on the clinical features, size, extent, and stage of the tumor.
- Lumpectomy: the portion of the breast that contains the cancerous cells is excised while leaving the remainder of the healthy breast tissue is left in place.
- Axillary lymph node dissection (ALND): removal of affected lymph nodes in the axillary region; the amount removed depends on the extent of the cancer spread.
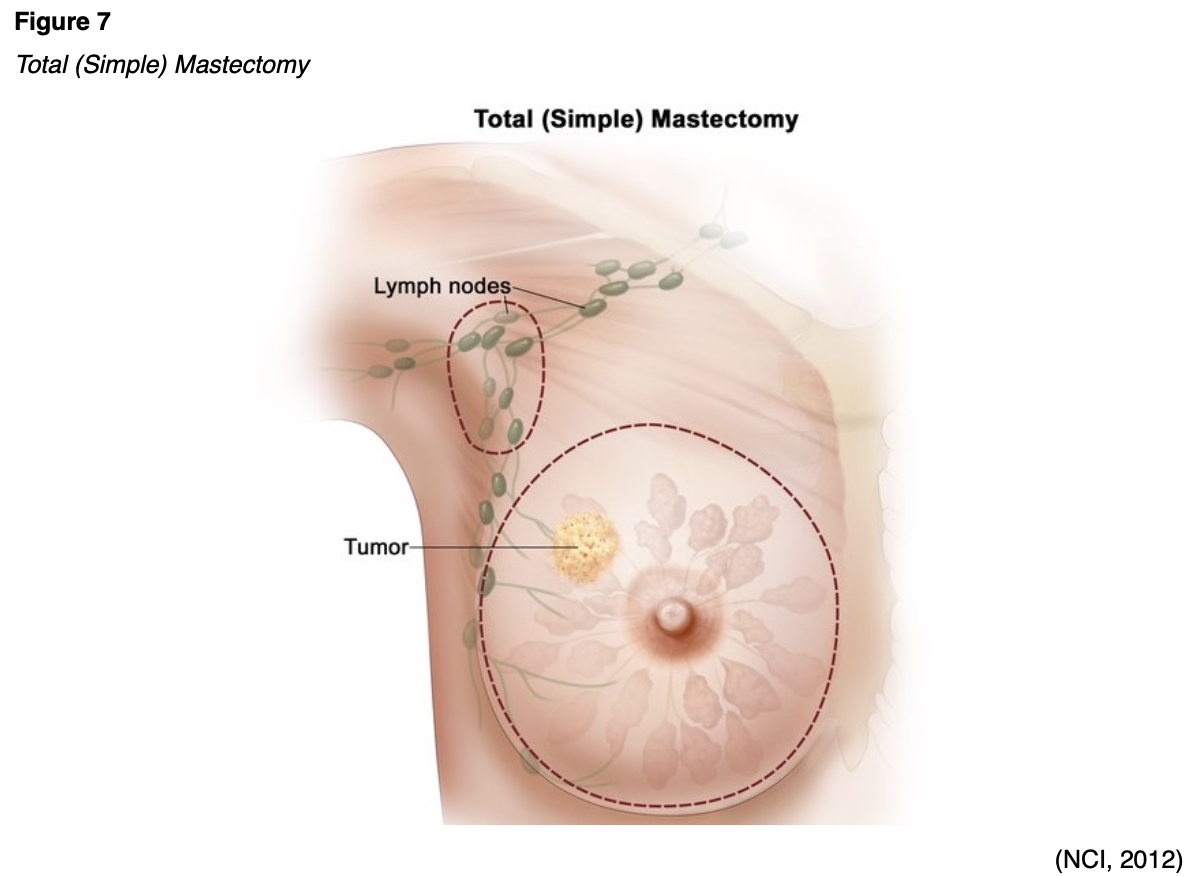
- Mastectomy:
- Total (simple) mastectomy: the breast tissue, nipple, areola, and skin are removed, but not all the lymph nodes. This procedure is demonstrated in Figure 7.
- Modified radical mastectomy: the entire breast and most of the axillary region and lymph nodes are removed, but the chest wall muscles under the breast remain.
- Radical mastectomy: the most extensive type of mastectomy in which the entire breast is removed, ALND, as well as the chest wall muscles under the breast.
- Partial mastectomy: the cancerous portion of the breast tissue is removed, along with some of the surrounding healthy tissue; this is very similar to lumpectomy, except more tissue is removed.
- Nipple-sparing mastectomy: all of the breast tissue is removed, except the nipple is spared.
- Prophylactic mastectomy: women with an increased risk for breast cancer due to BRCA1/2 genetic mutations or strong family history may consider bilateral prophylactic mastectomy as a risk reduction measure. Further, some women who have had cancer in one breast may also opt to have the other breast removed as a means of prevention (Breastcancer.org, 2020a).
Chemotherapy
Surgery for breast cancer may or may not be preceded by neoadjuvant chemotherapy or followed by adjuvant therapy. Neoadjuvant chemotherapy is administered to shrink a tumor so that the surgical intervention may not need to be as extensive. In breast cancer patients, neoadjuvant chemotherapy may shrink the tumor enough so that the breast surgeon may be able to perform a lumpectomy instead of a mastectomy. Adjuvant therapy is given following surgery to eradicate any micro-metastases and prevent cancer recurrence. Micro-metastases are a small collection of cancer cells too tiny to be identified on imaging scans that have detached from the original tumor and spread to other parts of the body. The danger with micro-metastases is that they can group together and form additional cancerous tumors within the body (Yarbro et al., 2018). Chemotherapy, also referred to as cytotoxic or antineoplastic therapy, encompasses a group of high-risk, hazardous drugs with the intent to destroy as many cancer cells with as minimal effect on healthy cells as possible. There is a wide range of chemotherapeutic agents used in breast cancer, and they are usually given in combinations of two or three drugs (Nettina, 2019).
Radiation Therapy
Radiation therapy is a localized treatment that uses ionizing radiation to treat cancerous tumors, with the primary objective of delivering a precisely measured dose of radiation to a defined tumor with as little injury as possible to surrounding healthy tissue. Radiation induces cellular damage to cancer cells, leading to biological changes in the DNA. This causes cells to die over days, weeks, and months, rendering them incapable of reproducing or spreading. All healthy cells and cancer cells are vulnerable to the effects of radiation and may be injured or destroyed. However, most healthy, non-cancerous cells can repair themselves and remain functional, whereas the cancerous cells are destroyed from the radiation (Yarbro et al., 2018). In breast cancer, radiation is generally performed following surgery to reduce the risk that cancer will return in the same breast, surrounding tissue, or lymph nodes. It may also be indicated for women following surgery if the tumor was large, if cancer cells were found in the lymph nodes, or if the surgical margins demonstrate signs of disease. Further, radiation therapy can also be used to control symptoms and for pain relief in patients with metastases in other parts of the body, such as the bones or the brain (ACS, 2019).
The two main types of radiation therapy used to treat breast cancer include external beam radiation therapy (EBRT) and brachytherapy. ERBT is the most common method used for breast cancer; it uses an external beam of radiation that is specifically focused on the targeted area. Brachytherapy is a form of internal radiation that is delivered through an implantable device that is placed inside the breast. Brachytherapy delivers targeted radiation to the tumor bed (or the location where cancer initially grew). Brachytherapy is often administered in only a few short treatments. Breast radiation is generally well-tolerated. The acute effects are usually transient, occur during treatment, limited to the skin, and generally subside within two weeks of treatment cessation. Nurses serve an important role with regards to educating patients on proper skincare during radiation, as up to 95% of patients will experience some degree of skin reaction (Nettina, 2019; Yarbro et al., 2018).
Hormonal Therapy
Hormonal treatments are targeted agents that work by blocking the hormones from reaching the cancer cells or by preventing the body from producing the hormones (Nettina, 2019). Estrogen and estrogen receptors are key drivers in many breast cancers, thereby making them amenable to hormone-blocking treatments to shrink or slow their growth. In addition to being a treatment option, hormonal therapy can also be administered as chemoprevention to lower the risk of ER/PR-positive breast cancer in individuals who are at high-risk but haven’t been diagnosed with breast cancer. Tamoxifen (Soltamax) is the oldest hormonal treatment for breast cancer. It is an estrogen agonist/antagonist that is given for the treatment of HR-positive breast cancers as well as a risk-reducing agent in patients with DCIS. Further, tamoxifen (Soltamax) is the most common agent used for chemoprevention in high-risk patients; the recommended duration of treatment is 5 to 10 years (FDA, 2018c). Currently, there are four major types of hormonal therapies, which are briefly reviewed in Table 3. The most common adverse effects of hormone treatment depend on the type of drug, but generally include hot flashes, night sweats, loss of libido, weight gain, joint aches or pains, mood changes, thinning or weakening of the bones (osteopenia or osteoporosis), and atrophic vaginitis (atrophy, loss of elasticity, dryness, and resulting irritation of the vaginal mucosa). Nurses should counsel patients on the importance of lifestyle behaviors and strategies to promote healthy bones, such as through adequate calcium intake and weight-bearing exercises (Olsen et al., 2019).

Targeted Therapies
Targeted therapies refer to a few classes of relatively novel treatment modalities that function by attacking specific parts of cancer cells to prevent tumor development or to shrink existing tumors. There are numerous proteins located on the cellular membranes called growth factor receptors, which connect the external and internal cellular environments and are essential for cell growth and development. These drugs can block or turn off chemical signals that tell the cancer cell to grow and divide, starve the tumor by cutting off blood supply and/or by preventing the formation of new blood vessels, or carry toxins or poison directly to the cancer cells, killing them without harming healthy cells (Sengupta, 2017). The development of specialized drugs that block these growth factor receptors has been a tremendous part of breast cancer research throughout the last few decades. These drugs have revolutionized treatment options for patients living with advanced and metastatic breast cancer by fighting against drug resistance and increasing survival. The next section provides a brief review of the major classes and types of targeted oral agents currently used to treat breast cancer (Breastcancer.org, 2020b; Masoud & Pages, 2017; NCCN, 2020).
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors
CDK4/6 inhibitors work by interrupting intracellular pathways and hormone signals that have roles in stimulating the growth and proliferation of cancerous cells (Scott et al., 2017). There are currently three CKD4/6 inhibitors approved by the FDA for use in combination with an aromatase inhibitor or fulvestrant (Faslodex) for women with HR-positive, HER2/neu-negative advanced or metastatic breast cancer, which include palbociclib (Ibrance), abemaciclib (Verzenio), and ribociclib (Kisquali). Nurses should counsel patients on the potential for adverse effects such as bone marrow suppression (neutropenia, anemia, and thrombocytopenia), diarrhea, and fatigue. Ribociclib (Kisqali) carries additional risks, including hepatobiliary toxicity and QTc interval prolongation, so patients should be advised that they will need to be monitored with blood tests and ECGs. (Shah et al., 2018).
Phosphatidylinositol-3-kinase (PI3K) Inhibitor
Worldwide, nearly 40% of HR-positive, HER2/neu-negative breast cancer patients have a PIK3CA mutation. Alpelisib (Piqray) works by inhibiting PI3K, which induces an increase in estrogen receptor transcription in breast cancer cells. This medication is given in combination with fulvestrant (Faslodex) to women who have PIK3CA-mutated breast cancer. Nurses should counsel patients on the most common side effects, which include diarrhea, nausea, fatigue, anorexia, and skin rash. The drug is also associated with severe adverse reactions, including hypersensitivity requiring drug discontinuation, severe skin reactions, hyperglycemia, and diarrhea. Patients require close monitoring of fasting blood glucose (FBG) and hemoglobin A1C (HbA1C) and may need to be started on an oral antihyperglycemic such as metformin (Glucophage) to optimize glucose control (Andre et al., 2019; FDA, 2019b).
Mammalian Target of Rapamycin (mTOR) Pathway
Everolimus (Afinitor) is an inhibitor of the complex mTOR pathway that is linked to many cancers. This medication is given in combination with an oral aromatase inhibitor. Nurses should educate patients that the most common side effect of everolimus (Afinitor) is oral mucositis, or inflammation, irritation, and swelling of the oral mucosa and lips, which can lead to painful mouth ulcers. Patients should be counseled on the benefits of practicing good oral hygiene to maintain the integrity of the oral mucosa, such as using a soft-bristled toothbrush and avoiding alcohol-based mouthwashes, as well as hot liquids and foods that can cause oral irritation and dryness. Additional reported side effects include fatigue, anorexia, skin rash, diarrhea, and increased serum cholesterol levels (FDA, 2018a).
Poly ADP-ribose Polymerase (PARP) Inhibitors
The PARP enzyme has a critical role in cell growth, regulation, and repair of both healthy cells and cancer cells. In cancer cells, it fixes DNA damage, essentially helping cancer cells repair themselves and survive (Olsen et al., 2019). Olaparib (Lynparza) is an oral medication that is used for women who have an inherited BRCA1 or BRCA2 mutation. The most common side effects include anemia, neutropenia, fatigue, nausea, diarrhea or constipation, anorexia, and arthralgias. Nurses should ensure patients understand that PARP inhibitors have several important drug interactions that can either decrease the effectiveness of the drug or cause serious toxicity. Some of the most common interactions include antifungal medications, certain antibiotics, grapefruit, and Seville oranges. Patients should be counseled on the importance of not starting new medications without first speaking to their clinician (FDA, 2018b; NCCN, 2020).
Monoclnal antibodies
Monoclonal antibodies are a type of targeted therapy that works by locating and attaching to specific receptors on the surface of cancer cells, such as the HER2/neu receptor. HER2/neu-positive breast cancer is amenable to HER2 directed monoclonal antibody treatments, such as trastuzumab (Herceptin) or pertuzumab (Perjeta). These agents are recombinant DNA-derived humanized monoclonal antibodies that selectively bind with high affinity in a cell-based assay to the extracellular domain of the HER2/neu receptor, inducing cell death. They are approved for treating patients with early-stage and advanced metastatic breast cancer whose tumors overexpress HER2/neu (Olsen et al., 2019). Trastuzumab (Herceptin) was the first drug approved by the FDA in 1998 for the treatment of HER2/neu-positive breast cancer. Trastuzumab (Herceptin) and pertuzumab (Perjeta) are intravenous infusions that may be used together or in combination with certain chemotherapy agents. They carry boxed warnings for cardiotoxicity, as they can lead to cardiac failure manifesting as decreased left ventricular dysfunction (LVEF) or congestive heart failure (CHF). Therefore, patients should be counseled on the need for cardiac monitoring with either an echocardiogram or multiple-gated acquisition [MUGA] scan at periodic intervals. It is also important that patients receive education on signs that may suggest possible cardiac dysfunction, such as shortness of breath, leg swelling, palpitations, reduced exercise tolerance, or dyspnea on exertion. Diarrhea is a common side effect of pertuzumab (Perjeta), with the incidence ranging from 28% to 72%; however, it can often be managed effectively without causing severe toxicity or drug discontinuation (Swain et al., 2017).
One of the most recent treatment developments targeting the HER2/neu gene is trastuzumab emtansine (Kadcyla), also called T-DMI. This is an antibody-drug conjugate of trastuzumab (Herceptin) that is linked to a cytotoxic agent. A conjugate is a compound that is combined with a chemotherapeutic agent as a means to induce a greater cell kill. Based on the KATHERINE trial, the risk of recurrence of invasive breast cancer or death was 50% lower with T-DM1 than with trastuzumab (Herceptin) alone (Minckwitz et al., 2019). Patients should be educated that this medication carries a boxed warning for hepatotoxicity, liver failure, and death, and they will require close monitoring of their liver function prior to each dose. The most common adverse reactions include fatigue, nausea, musculoskeletal pain, bleeding, headache, constipation, epistaxis, and arthralgias (FDA, 2019a).
Learn much more about these cancer treatment modalities, side effects, monitoring parameters, and nursing considerations with our Oncology Nursing CE courses and earn up to 10 ANCC credits.
The Early Detection of Breast Cancer
Breast Cancer Screening
Screening tests are performed to diagnose cancer before it grows large enough to cause symptoms and is still treatable or potentially curable. Early detection refers to finding and diagnosing the disease earlier than if the individual waited for the symptoms to develop. Breast cancers identified during screening exams are more likely to be small and still confined to the breast. The size of the tumor and whether or not it has spread are some of the most critical factors in predicting the patient’s prognosis, as tumor size at the time of diagnosis is directly related to mortality. Breast cancer screening is most commonly performed through mammography. Screening mammography beginning at age 40 saves the most lives and saves the most years of life, and annual screening saves more lives than every other year (biennial) (ACS, 2020a). Annual mammography screening in premenopausal women is associated with a significantly decreased risk of identifying advanced breast cancer than screening performed every other year. Postmenopausal women do not receive the same benefits of annual screening unless they are currently receiving hormone replacement therapy (HRT) for menopause; therefore, women 55 years or older can undergo screening every other year. The age to discontinue screening is not yet definitively established. Research demonstrates that continued screening may be beneficial in certain women 75 years or older, depending on their mortality risk, comorbidities, overall health, and performance status (CDC, 2018b). All women should be familiar with the known benefits, limitations, and potential harms of breast cancer screening. Women should check their breasts regularly to know how their breasts typically look and feel and report any breast changes to their healthcare provider immediately (ACS, 2020a; Smith et al., 2019).
High-Risk Women
Women who are known or likely carriers of the BRCA1/BRCA2 gene mutations and other high‐risk genetic syndromes or who have been treated with radiation to the chest for Hodgkin disease or other cancers are considered at increased risk. Annual screening mammography and MRI starting at age 30 are recommended for women in this high-risk category (ACS, 2020a; Smith et al., 2019).
Cancer Survivorship
According to the NCI Office of Cancer Survivorship (2020), “an individual is considered a cancer survivor from the time of diagnosis, through the balance of his or her life. There are many types of survivors, including those living with cancer and those free of cancer.” As of January 2019, there are an estimated 16.9 million cancer survivors in the US, representing approximately 5% of the population. Of these, 3.9 million (23%) are breast cancer survivors, and these numbers are both projected to rise over the next decade due to continued developments in research and technology (Miller et al., 2019; NCI Office of Cancer Survivorship, 2020). Nurses are uniquely positioned to facilitate survivorship care and improve the quality of care and patient outcomes. Nurses have the skills to integrate, coordinate care, and serve as patient educators and advocates. Nurses possess the skills and knowledge to assess and manage treatment-related side effects, provide education regarding the symptoms of recurrence, identification of late side effects, and the importance of adopting healthy lifestyle changes. Nurses must ensure that the patient has a knowledgeable primary care provider that specifically addresses survivorship needs and coordinates referrals to specialists as needed. The role of the nurse in survivorship can also significantly reduce the communication gap between providers and ensure cancer survivors are not lost to follow-up by facilitating communication between oncologists (Nettina, 2019).
Learn more about cancer prevention, early detection, and cancer survivorship with our NursingCE courses: Cancer Prevention and Early Detection (4 ANCC credits) and Cancer Survivorship (2 ANCC credits).
References
AbbVie Inc. (2019). Lupron depot® (leuprolide acetate for depot suspension). http://www.lupron.com/
American Cancer Society. (2019). Radiation for breast cancer. https://www.cancer.org/cancer/breast-cancer/treatment/radiation-for-breast-cancer.html
American Cancer Society. (2020a). American cancer society recommendations for the early detection of breast cancer. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
American Cancer Society. (2020b). Cancer facts & figures, 2020. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf
American Cancer Society. (2020c). Survival rates for breast cancer. https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-survival-rates.html
American College of Obstetricians and Gynecologists. (2017). Breast cancer risk assessment and screening in average-risk women. ACOG Practice Bulletin, 179, 1-16. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women.pdf
Andre, F., Ciruelos, E., Rubovszky, G., Compone, M., Loibl, S., Rugo, H. S., Iwata, H., Conte, P., Mayer, I. A., Kaufman, B., Yamashita, T., Lu, Y., Inoue, K., Takahashi, M., Papai, Z., Longin, A., Mills, D., Wilke, C., Hirawat, S., … SOLAR-1 Study Group. (2019). Alpelisib for PIK3CA-mutated, hormone-receptor-positive advanced breast cancer. New England Journal of Medicine, 380(20), 1929-1940. https://doi.org/10.1056/NEJMoa1813904
ANI Pharmaceuticals, Inc. (2019). Important safety information about Arimidex. https://www.arimidex.com/
Breastcancer.org. (2016). Lupron. https://www.breastcancer.org/treatment/druglist/lupron
Breastcancer.org. (2020a). Breast cancer stages. https://www.breastcancer.org/symptoms/diagnosis/staging
Breastcancer.org. (2020b). Targeted therapies. https://www.breastcancer.org/treatment/targeted_therapies
Breastcancer.org. (2020c). US breast cancer statistics. https://www.breastcancer.org/symptoms/understand_bc/statistics
BruceBlaus. (2014). Mammography [image]. https://commons.wikimedia.org/wiki/File:Blausen_0628_Mammogram.png
BruceBlaus. (2016). Breast biopsy [image]. https://commons.wikimedia.org/wiki/File:Needle_Breast_Biopsy.png
The Centers for Disease Control and Prevention. (2018a). What are the risk factors for breast cancer? https://www.cdc.gov/cancer/breast/basic_info/risk_factors.htm
The Centers for Disease Control and Prevention. (2018b). What is breast cancer screening? https://www.cdc.gov/cancer/breast/basic_info/screening.htm
The Centers for Disease Control and Prevention. (2019a). BRCA gene mutations. https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/brca_gene_mutations.htm
The Centers for Disease Control and Prevention. (2019b). Jewish women and BRCA gene mutations. https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/jewish_women_brca.htm
The Centers for Disease Control and Prevention. (2020). Breast cancer statistics. https://www.cdc.gov/cancer/breast/statistics/index.htm
Koh, J., & Kim, M. J. (2019). Introduction of a new staging system of breast cancer for radiologists: An emphasis on the prognostic stage. Korean Journal of Radiology, 20(1), 69-82. https://doi.org/10.3348/kjr.2018.0231
Masoud, V., & Pages, G. (2017). Targeted therapies in breast cancer: New challenges to fight against resistance. World Journal of Clinical Oncology, 8(2), 120-134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5385433/
McCance, K. L., & Heuther, S. E. (2019). Pathophysiology: The biologic basis for disease in adults and children. (8th ed.). Elsevier.
Miller, K. D., Nogueria, L., Mariotto, A. B., Rowland, J. H., Yarbroff, R., Alfano, C. M., Jemal, A., Kramer, J. L., & Siegel, R. L. (2019). Cancer treatment and survivorship statistics, 2019. CA: A Cancer Journal for Clinicians, 69(5), 363-385. https://doi.org/10.3322/caac.21565
Ill, G., Huang, C., Mano, M., Loibl, S., Mamounas, E., Untch, M., Wolmark, N., Rastogi, P., Schneeweiss, A., Redondo, A., Fischer, H., Jacot, W., Conlin, A., Arce-Salinas, C., Wapnir, I., Jackisch, C., DiGiovanna, M., Fasching, P., Crown, J., … Geyer, C. (2019). Trastuzumab emtansine for residual invasive HER2-positive breast cancer. New England Journal of Medicine, 380(7),617-628. https://doi.org/10.1056/NEJMoa1814017
National Breast Cancer Foundation. (2019a). Diagnosis. https://www.nationalbreastcancer.org/breast-cancer-diagnosis/
National Breast Cancer Foundation. (2019b). Types of breast cancer. https://www.nationalbreastcancer.org/types-of-breast-cancer/
National Cancer Institute. (2012). Total (simple) mastectomy [image]. https://commons.wikimedia.org/wiki/File:Total_(simple)_mastectomy.jpg
National Cancer Institute Office of Cancer Survivorship. (2020). Statistics, graphs, and definitions. https://cancercontrol.cancer.gov/ocs/statistics/index.html#definitions
National Comprehensive Cancer Network. (2020). NCCN clinical practice guidelines in oncology (NCCN Guidelines®) breast cancer version 5.2020 - July 15, 2020. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf
Nettina, S. M. (2019). Lippincott manual of nursing practice (11th ed.). Wolters Kluwer.
OncotypeIQ. (2020). About the oncotype DX breast recurrence score® test. https://www.oncotypeiq.com/en-US/breast-cancer/healthcare-professionals/oncotype-dx-breast-recurrence-score/about-the-test
Olsen, M., LeFebvre, K., & Brassil, K. (2019). Chemotherapy and immunotherapy guidelines and recommendations for practice. (1st Ed.). Oncology Nursing Society.
RadiologyInfo.org. (2018). General ultrasound. https://www.radiologyinfo.org/en/info.cfm?pg=genus
Raphseck. (2016). Breast cancer warning signs [image]. https://commons.wikimedia.org/wiki/File:Breast_cancer_illustration_en.svg
Scott, S. C., Lee, S. S., & Abraham, J. (2017). Mechanisms of therapeutic CDK4/6 inhibition of breast cancer. Seminars in Oncology, 44(6), 385-394. https://doi.org/10.1053/j.seminoncol.2018.01.006
Selchick, F. (2020). Breast cancer treatments [image].
Sengupta, S. (2017). Cancer nanomedicine: Lessons for immune-oncology. Trends Cancer, 3(8), 551-560. https://doi.org/10.1016/j.trecan.2017.06.006.
Shah, M., Nunes, M. R., & Stearns, V. (2018). CKD4.6 inhibitors: Game changes in the management of hormone-receptor-positive advanced breast cancer? Oncology (Williston Park), 32(5), 216-222. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6424488/pdf/nihms-1010845.pdf
Siegel, R. L., Miller, K. D., & Jemal, A. (2017). Cancer statistics, 2017. CA Cancer Journal for Clinicians, 67(1), 7-30. https://doi.org/10.3322/caac.21387
Simplyanon. (2011). Cancer staging [image]. https://en.m.wikipedia.org/wiki/File:Cancer_stages.png
Smith, R. A., Andrews, K. S., Brooks, D., Fedewa, S. A., Manassaram-Baptiste, D., Saslow, D., & Wender, R. C. (2019). Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA: A Cancer Journal for Clinicians, 69(3), 184-210. https://doi.org/10.3322/caac.21557
Swain, S. M., Schneeweiss, A., Gianni, L., Gao, J. J., Stein, A., Waldron-Lynch, M., Heeson, S., Beattie, M. S., Yoo, B., Cortes, J., & Baselga, J. (2017). Incidence and management of diarrhea in patients with HER2-positive breast cancer treated with pertuzumab. Annals of Oncology, 28(4), 761-768. https://doi.org/10.1093/annonc/mdw695
US Food & Drug Administration. (2017). Highlights of prescribing information: Faslodex® (fulvestrant). https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/021344s034lbl.pdf
US Food & Drug Administration. (2018a). Highlights of prescribing information: Afinitor®(everolimus). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022334s040,203985s013lbl.pdf
US Food & Drug Administration. (2018b). Highlights of prescribing information: Lynparza® (olaparib). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208558s001lbl.pdf
US Food & Drug Administration. (2018c). Highlights of prescribing information: Soltamox® (tamoxifen citrate). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021807s005lbl.pdf
US Food & Drug Administration. (2018d). MRI (magnetic resonance imaging). https://www.fda.gov/radiation-emitting-products/medical-imaging/mri-magnetic-resonance-imaging
US Food & Drug Administration. (2019a). Highlights of prescribing information: Kadcyla® (ado-trastuzumab emtansine). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/125427s105lbl.pdf
US Food & Drug Administration. (2019b). Highlights of prescribing information: PIQRAY® (alpelisib). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212526s000lbl.pdf
Watkins, E. J. (2019). Overview of breast cancer. American Academy of Physician Assistants, 32(10), 13-17. https://doi.org/10.1097/01.JAA.0000580524.95733.3
Yarbro, C. H., Wujcik, D., & Gobel, B. H. (Eds.). (2018). Cancer nursing: Principles and practice. (8th ed.)